Water Quality Basics
Is Tap Water Safe to Drink?
For most US households on regulated public water, the answer is usually yes. The real question is whether your water system, home plumbing, local advisories, or household needs create an exception.

For most people in the US on a regulated public water system, generally yes. For a healthy adult with no active violation, no advisory, and no obvious household risk like older lead-prone plumbing, tap water is unlikely to be a major added health risk. What decides your case is two things: legal versus health, and the system versus your home.
You have probably seen both claims: that US tap water is carefully regulated, and that you should never drink it unfiltered. Both can be true in specific situations, and neither describes every tap. The national picture is genuinely reassuring, and there are specific situations where it does not describe what comes out of your tap. People warn against tap water for real reasons (lead pipes in older homes, local advisories, private wells), but those reasons are specific, not universal. On this page, a claim counts as solid only when both a regulator and a mainstream scientist would call it fair. The goal is to show where that baseline holds and where it does not.
How safe is US tap water, really?
In fiscal year 2023, 92.4% of people served by US community water systems got their water from a system with no reported violation of EPA's health-based standards all year (EPA's Report on the Environment). That is a real, reassuring baseline. It is not the same as proof that every glass was risk-free.
Community water systems are the ones that serve the same homes year round, which is why this figure speaks to your kitchen tap more directly than the broader count that also folds in campgrounds and gas stations. More than 320 million people, roughly 95% of the country, get their water this way. "Health-based standards" is the plain-English shorthand for the EPA rules meant to protect health directly: a limit on how much of a contaminant is allowed (an MCL), a limit on disinfectant levels (an MRDL), and required treatment steps (a treatment technique). A system with no reported violation of any of those, across a full year, is the situation 92.4% of served people were in. That share has improved over time; EPA’s comparison point was 78.8% in fiscal 1993.
The figure describes systems and years, not individual glasses. "No reported violation" means a system stayed within those standards as measured and reported, not that the water was flawless at every address and every hour.
The same EPA source also shows where the year fell short, and it is worth seeing plainly rather than glossing over. The largest categories were surface-water treatment violations (systems serving 14.4 million people, 4.5%) and disinfection-byproduct violations (3.7 million, 1.2%); coliform-rule violations reached 2.7 million people (0.85%), and arsenic and nitrate violations were smaller still (312,800 and 175,300 people respectively). Those are real shortfalls, but they are concentrated in particular systems and years, not a sign that the baseline is hollow.
Two cautions keep that counterweight honest. When a system has a violation, EPA counts its entire service population even though only part of it may actually receive non-compliant water, so these exposure numbers can overstate how many people drank affected water; EPA itself notes there is no way to know how many, if any, people were truly drinking water in violation. And because a few systems are very large, a single one can move the national figure by two or three points in either direction. Separately, some systems fall short on monitoring or reporting (late, incomplete, or missing data) rather than on a health standard itself. That is tracked apart from confirmed health-based violations, but it can leave the picture less complete than a single percentage suggests.
So the honest reading of the baseline is steady, with gaps that matter. That clean compliance record answers the legal question. The health question is separate, and it comes next.
Does meeting the legal limit mean my water is healthy?
Not necessarily. EPA sets two numbers for many contaminants: an enforceable legal limit (the MCL) and a health goal (the MCLG). When they differ, the gap is usually about what treatment can achieve, measure, and afford, not a loophole or proof regulators stopped caring. So "within the limit" is not the same as "100% safe."

A report that shows no violations, like the national baseline above, is telling you a system stayed within its enforceable limits. That is real, and it matters. It is also a legal statement more than a complete health one. In plain terms, the health goal is the level EPA considers to carry no known risk, with a margin built in, and the enforceable limit is the line a system can actually be held to. Often the two are the same number. When they are not, it is usually because the health goal sits below what current treatment can reliably remove, or even measure, at a cost systems can bear. The law directs EPA to set the enforceable limit as close to the health goal as is feasible. The goal points to where the health science leads; the limit reflects what is achievable right now.
Arsenic is the cleanest illustration. EPA's enforceable limit is 10 micrograms per liter, the same figure the World Health Organization uses, but EPA's health goal for arsenic is zero (EPA National Primary Drinking Water Regulations; WHO arsenic fact sheet). That looks like a contradiction and is not one. WHO labels its own 10 a provisional value precisely because lower levels are hard to reach and hard to measure reliably, and EPA's limit reflects the same practical ceiling. The zero goal says no amount of arsenic is treated as free of risk; the enforceable 10 says that is the lowest point treatment can dependably hold today.
PFAS, the so-called forever chemicals, show the same split in a live and shifting form. In 2024 EPA finalized its first national PFAS drinking-water standards, six in all, and for two of them, PFOA and PFOS, set the enforceable limit at 4 parts per trillion against a health goal of zero (PFAS National Primary Drinking Water Regulation, Federal Register). As with arsenic, the zero is not a claim that any trace causes harm; it reflects EPA finding no level it can identify as risk-free, with the enforceable number set at what testing and treatment can currently manage.
The status here is in motion, so it is worth dating. As of June 3, 2026, all six of those 2024 standards remain final and on the books. EPA proposed two changes in May 2026: one proposed rescission rule that would roll back four of the six standards, and one proposed PFOA/PFOS compliance extension rule that would let certain systems request more time to meet the PFOA and PFOS limits. Both are proposals, not final rules, with comments due July 20, 2026. Unless and until something is finalized, the 2024 limits all still stand, including the standards proposed for rollback and the original compliance timing. (What these chemicals actually do at different exposure levels is a separate question, covered further down.)
This also explains how two official sources can publish different numbers for the same chemical without either being useless. A regulator setting an enforceable limit is answering what systems can be held to under the drinking-water law. A health agency may be answering a different exposure question, using a different time frame, endpoint, or safety assumption. Different questions can produce different numbers. Knowing which source is answering which question is its own skill.
If my city's water meets standards, is my tap safe?
No, not fully. A city or system meeting federal standards is necessary, but it does not settle what is true at your particular faucet. Compliance is measured across a whole system, while some of the biggest risks, lead especially, are added after the water leaves treatment, inside your service line and household plumbing.
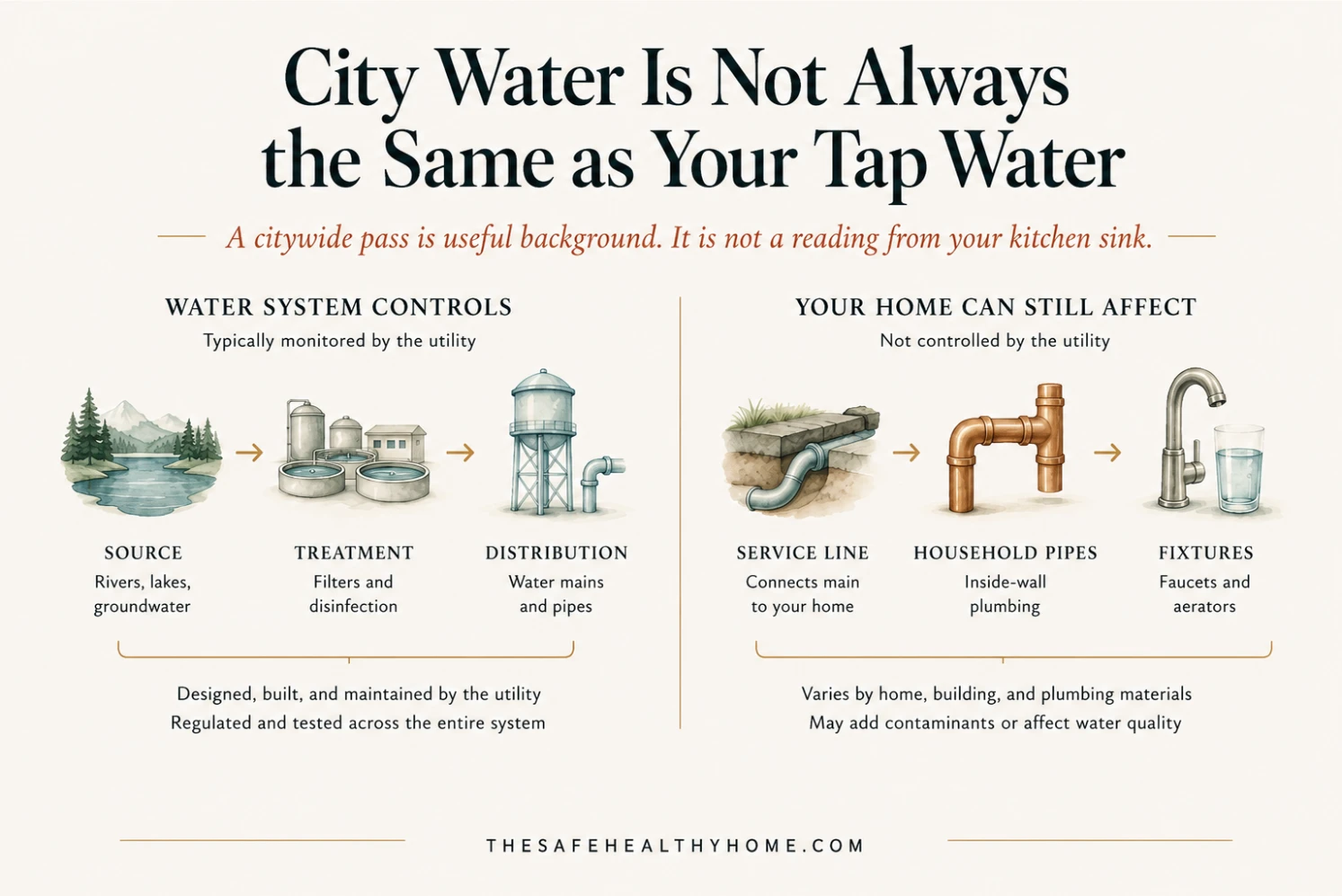
It helps to picture the water's path in two stretches. The first is the part your water system controls: the source, the treatment plant, and the large mains running through town. The second is the stretch closest to you, the service line into your building and the pipes, solder, and fixtures inside it. Federal standards are mostly tested and enforced on that first stretch. The second is largely on your side of the meter, and it is where the most common household problem appears.
Lead is where this gap matters most, and it is regulated unlike a contaminant such as arsenic for one main reason: it usually does not come from the source water at all. It enters later, when water meets lead service lines, lead solder, older brass fixtures, or galvanized pipe, and corrosion lifts some of it into what comes out of the faucet (EPA, Lead Service Lines). Because the lead is picked up so close to the tap, EPA cannot manage it with a single number measured at the treatment plant. So rather than a conventional enforceable limit, lead is handled through required treatment steps, mainly corrosion control, alongside a long-term program to locate and replace lead service lines. EPA's health goal for lead is zero. No level is treated as safe, and the concern is sharpest for young children and during pregnancy.
That structure is also why a system can be meeting the lead rules while a particular home still has elevated lead. Compliance is judged from a 90th-percentile figure. A system samples a set of higher-risk homes, and the rule looks at the level that 90 percent of those samples fall below; if that figure crosses a set threshold, called the action level, the system must strengthen corrosion control and take further steps. By design, then, up to a tenth of sampled homes can sit above that threshold while the system stays within the rules, and your home may share nothing with the homes that were sampled. A citywide pass is real information. It is not a reading from your kitchen sink.
These rules are mid-transition, which is worth knowing when you read anything local. EPA's Lead and Copper Rule Improvements are final and in effect, and they lower the lead action level to 10 parts per billion under the revised framework, down from the older 15 (EPA LCRI overview; Federal Register final rule). But most of the major obligations, including the schedule for replacing lead service lines, formally begin on November 1, 2027. Until then, your local water report may still describe lead using the legacy 15 ppb framework, so a current report and the newer standard can both be accurate while looking different. The rule is also being challenged in court by water-industry groups, which is a reason to keep an eye on its details, not a reason to discount the lead concern or to treat the rule as optional. It remains in effect.
In practice the takeaway is narrow and usable. If you live in a home built before 1986, when lead plumbing and solder were still common, if you do not know what your service line is made of, if you are mixing infant formula, if you are pregnant, or if you are uneasy about one specific fixture, then citywide compliance is useful background rather than a personal answer. Closing that gap is a local and household question: what your specific area and building tend to carry, and, where it is warranted, a direct test of the water coming out of your tap. For now, the important point is simpler: citywide compliance is useful context, but your home may still need its own answer.
Is tap water bad for you?
Not usually. For most healthy adults on a regulated public system with no active violations, advisories, or high-risk plumbing, tap water is generally safe to drink and unlikely to be a major added health risk. Risk concentrates around specific contaminants and specific people: infants, pregnant women, the immunocompromised, private wells, and lead-prone homes.
The useful version of this question is not "is tap water bad" but "under what conditions, and for whom." Most of the contaminants people worry about follow a pattern: at the low levels typical of a compliant system, they are usually not a major added risk for most healthy adults, while at an exceedance, during an advisory, or with years of higher exposure they matter much more. That is the legal-versus-health and system-versus-home split from above, now applied to your body. The contaminants below are the ones worth understanding, each with its real level of concern stated plainly.
Disinfection byproducts
When a water system adds chlorine or a similar disinfectant to kill germs, a small share of it reacts with natural organic matter already in the water and forms new compounds. Two regulated groups, trihalomethanes (TTHM) and haloacetic acids (HAA5), are the most closely watched. The concern with them is mainly long-term: exposure above the limits over many years has been associated with a possible increase in cancer risk and with liver, kidney, or nervous-system effects (EPA National Primary Drinking Water Regulations).
Disinfection is one of the main reasons waterborne disease is uncommon in regulated US systems, and the rules try to keep byproducts low without weakening protection against germs. So this is a long-term balance a system manages, not a reason to fear chlorinated water or to want disinfection stopped. The limits exist to keep the byproducts low while the disinfection keeps doing its job.
PFAS
PFAS, a large family of long-lasting industrial chemicals, are a real long-term concern, and also a place where a single detection is easy to misread. EPA's current understanding links certain PFAS exposures to increased risk of some cancers (including kidney, testicular, and prostate), reduced immune and vaccine response (the most sensitive effect, and one seen in children), reproductive and developmental effects including lower birth weight, thyroid and hormone disruption, and higher cholesterol (EPA, Our Current Understanding of the Human Health and Environmental Risks of PFAS).
That list comes with two honest qualifiers. EPA has not set a cancer-risk concentration in water for PFOA or PFOS, because those cancer analyses are still ongoing. And the health goal of zero does not mean any detectable amount causes harm; it means EPA has not identified a level it can call risk-free, which is a different statement. As covered earlier, all six of the 2024 PFAS standards remain final as of June 3, 2026, with the May 2026 changes still only proposals. If your water report or a local source flags PFAS, that is a reason to learn your actual numbers and act on them, not a reason to assume harm has already occurred.
Nitrate
Nitrate breaks the usual pattern, because its most serious risk is acute rather than slow. EPA's limit is 10 milligrams per liter, measured as nitrogen (EPA Chemical Contaminant Rules). The group at real risk is narrow but important: infants under about six months, mainly when formula is mixed with high-nitrate water. In those infants, nitrate can interfere with the blood's ability to carry oxygen, a condition called methemoglobinemia, or "blue-baby syndrome," which can become serious or fatal without prompt care. Older children and adults are far less sensitive.
Nitrate is also a know-your-local-water contaminant rather than a national worry. It concentrates where fertilizer runoff, septic systems, and animal waste reach groundwater, which puts agricultural areas and private wells at the front of the line.
One warning is important enough to state plainly: do not boil high-nitrate water to make it safer for infant formula. Boiling does not remove nitrate, and it actually concentrates it as water evaporates. If high nitrate is a possibility, use a different, known-safe water source for formula and contact your water provider or local health department.
Microbial contamination and boil-water advisories
Microbial contamination, from bacteria, viruses, or parasites, is one of the clearest short-term drinking-water risks, and it is the main reason advisories exist. A boil-water advisory is often precautionary: it can be issued when water is, or simply could be, contaminated after a main break, a loss of pressure, a treatment problem, or flooding, not only when contamination has been confirmed. It does not mean everyone has already been drinking unsafe water.
It helps to know the three kinds of advisory, because each calls for a different response (CDC, Drinking Water Advisories: An Overview). A boil-water advisory means boiling will make the water safe to use. A do-not-drink advisory points to something boiling will not fix, often a chemical, so bottled water is used for drinking and cooking until it lifts. A do-not-use advisory means avoiding the water altogether, including for washing, until it is cleared.
When boiling is the instruction, the guidance is a rolling boil for one minute, or three minutes above 6,500 feet of elevation. Boiling reliably kills viruses, bacteria, and parasites. It does not remove chemical contaminants, which is exactly why the do-not-drink and do-not-use categories exist.
Lead
Lead belongs on this list too, but it is the clearest case of household-specific rather than system-wide risk, so the detailed explanation belongs in the earlier section on whether your city’s compliance reaches your tap. The short version: it matters most for young children and during pregnancy, and because it usually enters from home plumbing and service lines, the real question is about your home, not the national average.
Two quick notes round out the picture. Fluoride is not a simple good-or-bad contaminant: US public-health agencies still recommend community fluoridation around 0.7 mg/L for cavity prevention, while newer neurodevelopmental reviews raise concern mainly at higher total exposures, especially above about 1.5 mg/L; that trade-off deserves its own full guide.
And because filters come up constantly with these contaminants, it is worth saying clearly: a filter is not a substitute for knowing the contaminant, but when testing, a CCR (your annual local water report), a lead service line, or an advisory points to a specific risk, a certified filter can be the right interim tool. Matching a filter to a particular problem is a separate decision.
Why does my tap water taste, smell, or look off, and is that dangerous?
Usually not an emergency. Most taste, smell, and appearance changes are aesthetic or tied to the system, not a sign your water is unsafe to drink. A few deserve action, though: sudden discoloration, a sewage or chemical smell, any change during a known advisory, or symptoms after drinking. Gross and dangerous are not the same.
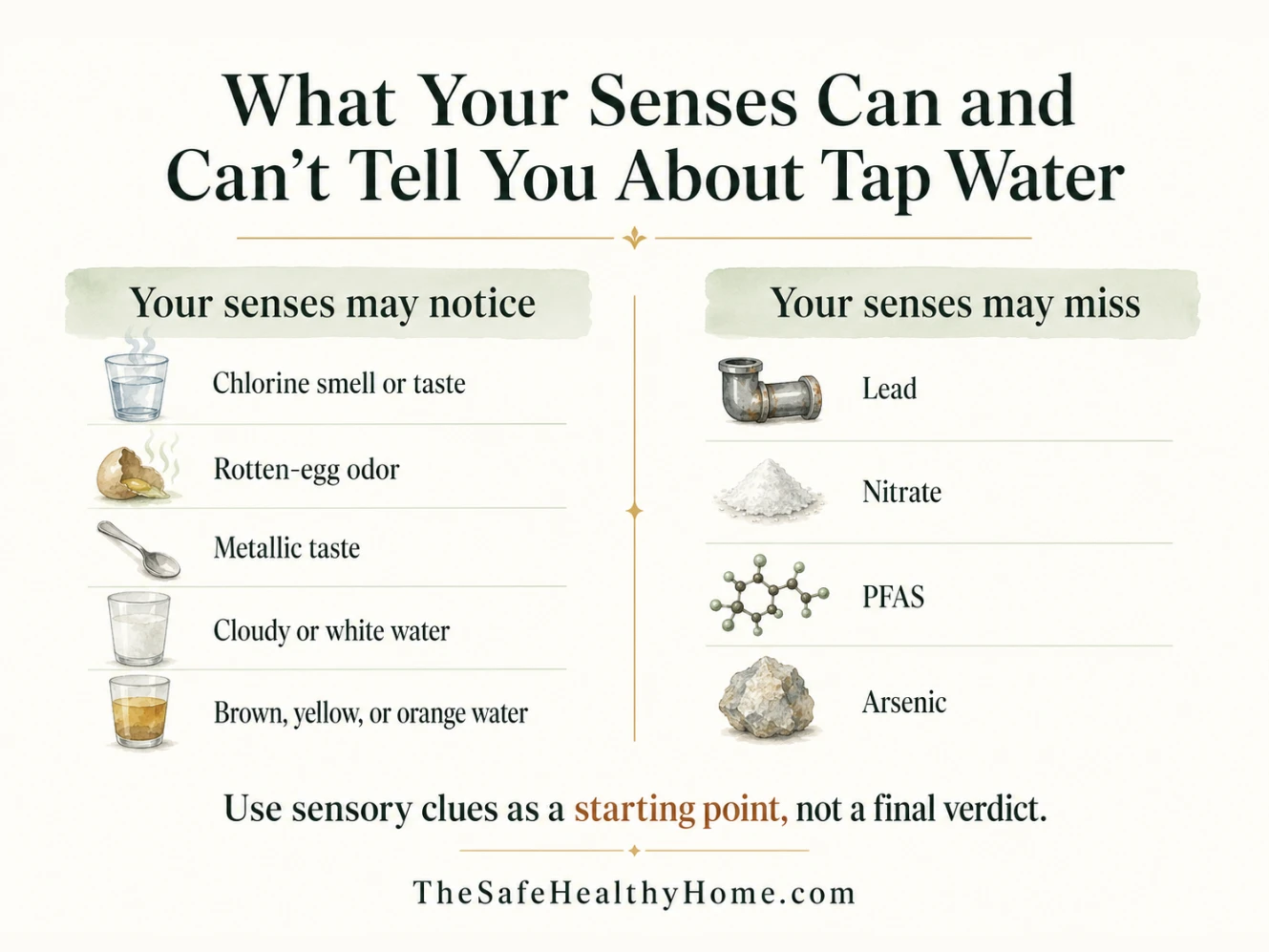
Your senses are good at catching changes and bad at diagnosing them. A new taste or color tells you something shifted; it rarely tells you what, and it almost never tells you whether the water is harmful. Use the cues below as a starting point, not a verdict. EPA’s secondary drinking-water standards also treat many taste, odor, color, and staining issues as aesthetic indicators rather than health standards (EPA secondary drinking water standards).
| What you notice | What it often points to | Aesthetic or worth a closer look | What to do |
|---|---|---|---|
| Chlorine or "pool" smell or taste | The disinfectant residual the system carries through the pipes | Usually aesthetic | If it bothers you, chill water in an open pitcher and the smell often fades. By itself, not usually a reason to stop drinking it. |
| Rotten-egg or sulfur smell | Hydrogen sulfide, often from the water heater if it is only in hot water, or from groundwater and well sources | Usually aesthetic, but a sewage-like smell is different | If it is only in hot water, suspect the heater. If it is in cold water too, or smells like sewage, contact your water provider. |
| Metallic taste | Iron or copper, or water that is corroding household plumbing | Usually aesthetic, but can be a corrosion clue | In an older home, treat it as a reason to consider a lead-and-copper test, not as a diagnosis. |
| Cloudy or white water | Tiny air bubbles, common in cold weather or after work on the line (USGS) | Usually aesthetic | Fill a glass and let it stand. If it clears from the bottom up within a minute or two, it was air. If it stays cloudy, contact your provider. |
| Brown, yellow, or orange water | Iron, rust, or stirred-up sediment, often after hydrant flushing or a main disturbance | Usually aesthetic, but worth a call if sudden or widespread | Run the cold tap a few minutes to see if it clears. Avoid using discolored water for laundry or infant formula until it runs clear. If it persists, contact your provider. |
There is one real limit on all of this: the contaminants most worth worrying about give no warning to your senses. Lead, nitrate, PFAS, and arsenic are typically invisible, odorless, and tasteless at the levels that matter. Clear, pleasant water can still carry them, and unappealing water is often harmless. That is why a real answer comes from your local report and, where warranted, a test, not from the glass in front of you. If a concern is specific enough to matter, the next step is testing for that concern. If a test turns something up, then choosing a filter should be based on that specific result.
What if I have a private well?
The national baseline does not apply to you. EPA regulates public water systems, but it does not regulate private household wells, so no agency is monitoring your water or reporting violations on your behalf. Testing it, maintaining it, and deciding whether it needs treatment are the owner's responsibility.
A private well can be excellent water, and many are. But "excellent" and "verified" are different things, and a well is not covered by the monitoring, treatment requirements, and annual public reporting that sit behind a community water system (EPA, Private Drinking Water Wells). The national baseline from the top of this page simply does not describe it.
What a well is exposed to depends on local geology and what sits nearby. The common concerns are bacteria, nitrate, and arsenic, and the odds rise with agricultural runoff, septic systems, flooding, and nearby land use. None of these announce themselves at the tap, which is the same lesson as the section above: you find them by testing the water, because taste alone cannot reveal them.
At a minimum, most guidance points to testing a private well at least once a year for bacteria and nitrate, with added tests for arsenic or other local concerns depending on your area's geology and land use. If you are mixing infant formula, the nitrate point from earlier applies directly and is worth acting on rather than assuming. The specifics of what to test for and how often depend on your well, your area, and nearby land use.
Is bottled water safer than tap?
Not categorically. Bottled water is regulated differently, not automatically better or worse. FDA standards generally track EPA contaminant standards, but testing, source protection, public reporting, cost, plastic exposure, and emergency usefulness differ. So the honest answer depends on your situation rather than on the fact that it came in a bottle.
The difference starts with who is in charge. EPA regulates public tap water under the Safe Drinking Water Act, while the FDA regulates bottled water as a packaged food. By law, the FDA's bottled-water standards must be at least as protective of public health as the EPA's, and they match EPA's limits for dozens of substances; on lead, the bottled standard is actually stricter than the tap limit (FDA, FDA Regulates the Safety of Bottled Water).
In practice, though, oversight of bottlers is looser in several ways. A 2009 GAO review found bottled-water protections were often less stringent than comparable tap-water protections: bottlers test less frequently than large municipal systems, there is no equivalent mandate to protect the source water, and bottled water sold only within one state can fall outside federal oversight entirely (GAO). The source is sometimes the same water. By NRDC's estimate, a quarter or more of bottled water starts as municipal tap water, sometimes treated further and sometimes not, though the exact share is debated (NRDC).
So bottled water is not a routine upgrade just because it comes sealed in plastic, and it carries a higher cost and environmental footprint. Where it earns its place is specific and short-term: during an active boil-water or do-not-drink advisory, when a household has a known lead problem, or for an immunocompromised household during an advisory. Plastic exposure, including microplastics, is a real and active question, but it belongs with the fuller comparison rather than here. For this page, the key point is enough: bottled water can be useful in specific situations, but it is not automatically a better everyday answer.
Who should you believe when the sources disagree?
Usually, sources disagree because they are answering different questions. Regulators like EPA set enforceable floors, the limits a system can be held to. Health agencies may focus on health effects, exposure context, or screening values. Advocacy groups may focus on lower health-based targets or worst-case concerns. Neither is lying; the trick is knowing which question a given number is answering.
A simple ranking helps, less as a pecking order than as a map of what each source is for.
Start with EPA's enforceable standards, and with your local water report as their local form. These tell you whether your system is actually meeting the limits it can be held to. That is the legal floor, and it is the most concrete thing you have.
Next come the health goals: EPA's own MCLGs, and the World Health Organization's health-based guidelines where they differ, as with arsenic. These describe where the health science points, separate from what is enforceable today. They are why "within the limit" and "no known risk" can be different statements.
Then there are the federal health agencies, the CDC and ATSDR, which publish health context and screening values, often for emerging concerns like PFAS. These sources help explain health effects, exposure context, vulnerable groups, and screening values, which is different from saying what a water system can be held to under the drinking-water law.
Advocacy sources like the Environmental Working Group belong on the map too, as useful context rather than the final word. EWG's database often looks far more alarming than an EPA table, and the reason is not dishonesty: it measures against its own health-based targets, which sit well below enforceable limits, and it leans toward flagging concern early. Local news works similarly, surfacing real problems while compressing the nuance. Treat both as a prompt to look closer, not as the verdict itself.
One test holds the hierarchy together. Before trusting a framing, ask whether both an EPA scientist and a mainstream toxicologist would call it fair. A claim only one camp would endorse, in either direction, is a signal to slow down. Different sources can each be useful without being interchangeable, and the skill is matching the source to the question you actually have. When you are ready to move from “is tap water generally safe?” to “what should I check in my own water?”, the Home Water Quality hub gives you the step-by-step path: source, local report, testing, interpretation, and treatment decisions.
How do I find out if my tap water is safe?
Three steps, in order. First, identify your situation, since a city apartment, an older house, a private well, and a household with an infant each start in a different place. Second, read your local water report. Third, test, but only when your situation actually calls for it rather than by default.
Identify your situation
| Your situation | What the baseline means | First step | When to go further |
|---|---|---|---|
| Public-system city dweller | The national baseline mostly applies; your system is monitored and reports yearly | Read your CCR and note any violations or lead action-level exceedances | If your building is older, your household is vulnerable, or the CCR flags something |
| Older home or unknown service line (built before 1986, or lead-prone plumbing) | System compliance does not settle lead at your tap, since lead is added after treatment | Find your service-line material (your provider may have a locator) and consider a lead-and-copper test | Sooner if there are young children, a pregnancy, or formula-feeding in the home |
| Private well | The federal baseline does not apply; no agency monitors or reports for you | Test at least once a year for bacteria and nitrate | Add arsenic and other local-risk tests based on geology, agriculture, septic systems, or flooding nearby |
| Vulnerable household (infants, pregnant women, immunocompromised, anyone mixing infant formula) | The national baseline may still apply, but the stakes are higher and some contaminants matter more | Read the CCR and pin down lead and nitrate risk specifically | Use a known-safe source for infant formula if nitrate is possible, and test rather than assume |
Read your local water report
For anyone on a public system, the first document to find is your Consumer Confidence Report, or CCR: the annual drinking-water quality report your provider is required to publish (EPA, Consumer Confidence Reports). It is usually available online, and public systems must provide it to customers at least once a year.
A handful of things are worth locating in it: which contaminants were detected and at what levels, any violations during the year, the enforceable limits (the MCL) alongside the health goals (the MCLG), the lead action level, where your water comes from, and the standard health language about vulnerable groups.
Reading it well is mostly about avoiding a few common misreads. A detected contaminant is not automatically unsafe; detection just means it was measurable, often far below the limit. "No violations" is reassuring but does not mean zero risk, for the legal-versus-health reason from earlier. The MCL and the MCLG often differ. And the report describes the system as a whole, not the water at your particular faucet, which is exactly why an older home may still want a test even when the CCR looks clean.
Good, better, best: a testing ladder
When testing makes sense, picture three rungs.
Good is free: your CCR or local water report, which answers the system-level question for most public-system households with no special concern.
Better is a low-cost screening kit, roughly $20, useful for a quick read on a limited set of questions. These strips are a screen, not a verdict. They are coarser than lab testing and easy to misuse, so treat a worrying strip result as a reason to test properly, not as a diagnosis.
Best is a certified lab panel, roughly $150, which is the right call when the stakes are higher or when the contaminant cannot be judged by taste, smell, or appearance: an older home or lead-service-line concern, a private well, infant formula and nitrate, or any home after a local advisory or a recent water-quality problem.
A filter is not a substitute for knowing the contaminant. But when testing, a CCR, a lead service line, or an advisory points to a specific risk, a certified filter can be the right interim tool. The main point is to avoid guessing: test for the concern first, then match any filter decision to that result.
The honest bottom line
So, is tap water safe to drink? For most people in the US on a regulated public water system, the honest answer is generally yes, and that is not a polite dodge. The national baseline is real, and decades of treatment, monitoring, and regulation are a major reason tap water is rarely a major added health risk for a healthy adult.
The answer changes in specific, knowable situations: when your system has an active violation or advisory, when an older home carries lead-prone plumbing, when the household includes an infant, a pregnant woman, or someone immunocompromised, or when you are on a private well that no agency is watching for you. None of those are cause for alarm. They are cause for a second look.
That is the whole article in two distinctions. Meeting the legal limit is meaningful, but it is not the same as matching the health goal. And a compliant system tells you about the network, not about the water at your faucet. Hold both in mind and the question stops being "is tap water safe" in general and becomes "is mine safe for my household," which is a question you can actually answer. The method is the same throughout: start with the system, check the household factors, and use testing when the answer needs to be specific.
Frequently asked questions
Why do people say not to drink tap water?
Usually for specific, real reasons rather than a blanket truth: lead plumbing in older homes, local advisories, private wells that no one monitors, PFAS where it has been detected, taste or smell complaints, and a general distrust of official sources. Each is a genuine concern in the right context. None of them means all tap water is unsafe, so the practical step is figuring out which, if any, is true where you live.
Is tap water 100% safe to drink?
No drinking water is 100% risk-free, and neither is bottled. That is the wrong standard to hold it to. The useful question is whether your system is meeting its standards and whether your home or household adds a specific risk, such as lead-prone plumbing or a formula-fed infant. "Within the limits" and "zero risk" are different claims, and honest sources do not promise the second.
Is indoor tap water safe to drink?
Usually, if it comes from a regulated public system with no current advisory and no household-specific risk. The wrinkle is indoors: a building's own plumbing can change the water after it arrives, lead being the main example. So "the city's water is fine" and "the water at this sink is fine" are not automatically the same thing, especially in older buildings.
How unhealthy is tap water?
For most healthy adults on a compliant, regulated public system, it is not usually a major added health risk. The concern rises in specific places: particular contaminants above their limits, systems with violations, private wells, lead-prone homes, and vulnerable households. For a healthy adult, the day-to-day risk is usually small; what moves the answer is a specific issue at your address or in your household, which is the thing worth checking.
Is fluoride in tap water bad?
Not a simple yes or no. US public-health agencies recommend community fluoridation around 0.7 mg/L for cavity prevention; the concern in newer neurodevelopmental reviews is mainly at higher total exposures, especially above about 1.5 mg/L. That trade-off deserves its own full guide.
Is it safe to drink tap water every day?
For most people on a compliant, regulated system, yes. Many drinking-water limits are designed with regular use in mind, not just a single glass, while advisories and acute contaminants are handled differently. The exceptions are about chronic conditions: an ongoing violation, a standing advisory, a private well, lead exposure risk at home, or certain vulnerable households. If one of those applies, daily use is exactly why it is worth checking.
Is tap water safe for babies or during pregnancy?
For formula-fed infants, the two practical concerns are nitrate and lead. Do not boil high-nitrate water to make it safer for formula, since boiling concentrates nitrate; use a known-safe source instead. Pregnant women have reason to pay attention to lead, to PFAS where it has been flagged locally, and to any advisory. This is a check-your-local-report-and-test situation rather than a reason to panic, and your local health department's guidance should lead.
Why does my tap water smell like chlorine?
Usually that is the disinfectant residual the system carries to keep water safe in the pipes, and it is generally aesthetic rather than a health problem. Chilling water in an open pitcher lets the smell fade. If the smell is sudden, very strong, distinctly chemical, or paired with an advisory or with symptoms after drinking, contact your water provider.
Who should I trust about whether my tap water is safe?
Match the source to the question. For whether your system is meeting enforceable standards, use EPA rules and your local CCR. For health context, the CDC and ATSDR. For advisories, your local health department. Advocacy groups like EWG are useful for early warning and pressure, not as a standalone verdict. And for the one question none of them can answer, what is true at your specific tap, the answer is a test.